Abstract
Background. The problem of the treatment of anxiety-depressive disorders in chronic pain is not solved, considering the significant somatization of psychopathological manifestations in dorsalgia and fibromyalgia; triggering and aggravating role of stress; lack of clear clinical recommendations for the management of patients with combined disease states.
Methods and materials. 164 patients with anxiety-depressive disorders and chronic pain were divided into the study group (n=81) with fibromyalgia and the comparison group (n=83) with joint pain (M25.5) or dorsalgia (M54 .0-9). Both groups were randomized into psychotherapeutic or pharmacotherapeutic treatment: F-Ph (fibromyalgia patients, psychopharmacotherapy - 42 persons), F-Ps (fibromyalgia patients, psychotherapy - 39 persons), JD-Ph (joint pain/dorsalgia patients, psychopharmacotherapy - 45 persons) JD-Ps (joint pain/dorsalgia patients, psychotherapy - 38 persons).
Psychopharmatherapy included SSRIs, SNRIs, and pregabalin in standard dosages according to the instructions. Psychotherapeutic interventions involved the following methods: psychoeducation, progressive muscle relaxation, rational therapy, art therapy, elements of cognitive behavioral therapy. Evaluating the effectiveness of the treatment was carried out at week 4 and 12 with Hamilton anxiety and depression scales (HAM-A and HAM-D).
Results. At week 4 of treatment, the most significant reduction in anxiety and depression symptoms occurred in psychopharmacotherapy groups, compared to psychotherapy. In particular, in patients with fibromyalgia (13.5 vs. 7.8, p=0.026 and 8.2 vs. 5.9, p=0.048, respectively).
At week 12 (end of treatment), there wasn't noted any significant difference between the effectiveness of pharmacotherapy and psychotherapy interventions for reducing anxiety and depression symptoms.
Conclusion. These data indicate the similar effectiveness of pharmacotherapy and psychotherapy in the treatment of anxiety and depression symptoms in patients with chronic pain.
Background
The treatment of anxiety and depressive disorders in patients with chronic pain in recent years is in the focus of global medical community 1,2,3,4. Association between anxiety-depressive disorders with varying degrees of severity, from phenomena to disorders, and chronic pain is described for traumatic, inflammatory and neurodegenerative lesions of the musculoskeletal and nervous system 5,6,7,8. Eventually, under the broad range influence of etiopathogenetic factors, some psychopathological symptoms tend to exacerbate, to form resistance to treatment and to chronicize, which can lead to profound worsening quality of life 9,10,11,12.
However, the data about psychosomatic relations in clinical settings, when etiopathogenesis of chronic pain is not entirely understood, e.g., in dorsalgia and fibromyalgia, remain controversial. On the one hand, under these conditions, psychosocial factors are often considered as having the leading role in disease progression. These factors include stressful events, pain limitations in daily activities, avoidant coping strategies, pain catastrophization, anxiety, depression, addictive behavior patterns, etc. 13,14,15,16. Conversely, on the background of views about a single neuroendocrine control system and its regulation of organism’s response, there are a lack of data about morphological and functional aspects of chronic pain 17,18,19.
Management of patients with dorsalgia in Ukraine is regulated by the Ministry of Health Decree #487 from 17.08.2007 “On approval of clinical protocols of medical care in Neurology”. As for the management of patients with fibromyalgia, there is acting Decree #311 from 25.04.2012 “On approval and introduction of medical and technical documents to standardize palliative medical care for chronic pain syndrome”, which includes a unified clinical protocol developed on the basis of adapted clinical guidelines on pain control (2012) 20,21. However, the problem of diagnosis and treatment of anxiety and depressive disorders in chronic pain is not solved, considering the significant somatization of psychopathological manifestations in dorsalgia and fibromyalgia; triggering and aggravating role of stress; lack of clear clinical recommendations for management of patients with comorbid diseases 22,23,24,25,26,27. Given the difficult social circumstances in Ukraine in recent years, we can suggest that the incidence of fibromyalgia and dorsalgia will rise, which gives clear relevance for studies in mental and psychosomatic disorders in patients with chronic pain.
Therefore, determining the optimal treatment tactics in anxiety and depressive disorders in patients with chronic pain due to diseases of the musculoskeletal system and connective tissue, e.g., dorsalgia and fibromyalgia, can contribute to more efficient treatment of such patients.
Methods and materials
The study was conducted at Institute of Neurosurgery, Ukraine. Overall, during 2011-2015 a total number of 218 patients with chronic pain due to musculoskeletal and connective tissue diseases have been surveyed at the Restorative Surgery Department.
Inclusion criteria: informed consent to participate in the study; age 18-65 years; chronic pain syndrome (HPS) of undetermined origin within the class M categories according to ICD-10 (M25.5 — joint pain; M54.0-9 — dorsalgia; M79.0 — fibromyalgia); the severity of chronic pain VAS scale ≥ 5 points; clinically significant anxiety and depression symptoms according to baseline HAM-A and HAM-D scores.
Exclusion criteria: HPS inflammatory, degenerative and traumatic origin within other class M categories according to ICD-10; psychotic condition, dementia, personality disorders, mental and behavioral disorders due to substance use; clinically significant other somatic disorders; failure to comply with the study settings.
It should be noted that all participants were included into the study after signing the informed consent, which had been pre-designed in accordance with principles of bioethics.
Taking into account inclusion/exclusion criteria and drop-outs during the study, final sample, which was included into analysis, comprised of 164 patients. From this sample, 81 patients were diagnosed with fibromyalgia (M79.0) and 83 — with HPS due to joint pain (M79.0) or dorsalgia (M54.0-9). They were randomized into one of two groups for treating with pharmacotherapy or psychotherapy. The analysis was conducted separately according to the diagnosis, whether the patient had fibromyalgia or chronic pain with other etiology. First two groups included patients with fibromyalgia, treated with psychopharmacotherapy (F-Ph, n=42) or psychotherapy (F-Ps, n=39), two comparison groups included patients with joint pain or dorsalgia, treated with psychopharmacotherapy (JD-Ph, n=45) or psychotherapy (JD-Ps, n=38).
Psychopharmacotherapy was prescribed depending on the disease’s clinical picture. Prescribed medications included SSRIs (sertraline, escitalopram, paroxetine), SNRIs (venlafaxine, duloxetine) and pregabalin in standard dosages according to the instructions. Psychological interventions included the following methods: psychoeducation, progressive muscle relaxation, and cognitive-behavioral therapy. They were delivered once a week with a total duration of 12 weeks.
Treatment effectiveness evaluation was conducted at week 4 and the end of final week 12. Differences between groups were assessed by calculation of Mean Difference ± Standard Deviation.
Results
Anxiety changes during the treatment
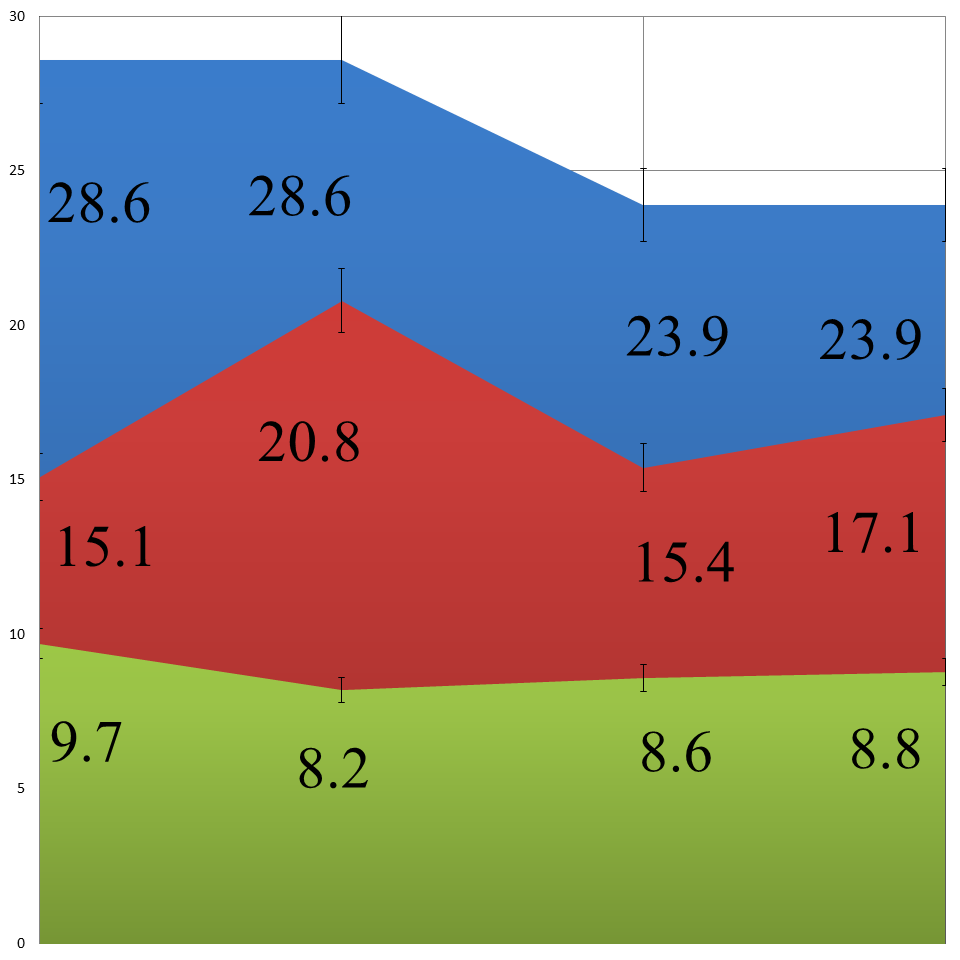
The mean HAM-A scores at the start of the treatment in F and JD groups was 28.6 ± 6.4 and 23.9 ± 6.3 respectively. At week 4 of treatment the most significant reduction in anxiety symptoms was observed in groups, treated with psychopharmacotherapy. Namely, in F-Ph and JD-Ph overall scores on HAM-A scale were 15.1 ± 4.3 and 15.4 ± 4.2 points respectively. Improvements were also noted in patients, assigned to psychotherapeutic interventions, but they were less significant. In particular, at week 4 in F-Ph group mean HAM-A score was 20.8 ± 5.8, and in JD-Ps — 17.1 ± 5.6 points. There was noted statistically significant difference between psychotherapy and pharmacotherapy groups in favor of latter (p<0.05).
At week 12, at the end of the treatment, the most pronounce reduction of anxiety symptoms was noted in patients, assigned to the psychological interventions. Particularly, the overall mean HAM-A score was lower in F-Ps group (8.2 ± 3.6 points), than in F-Ph group (9.7 ± 3.7 points). As for JD patients, there weren’t any significant differences noted between treatments. In long-term treatment anxiety have reduced to HAM-A mean score of 8,6 ± 3,4 points in JD-Ph and 8,8 ± 3,6 points in JD-Ps group. Moreover, in most of the patients from all groups anxiety remained at a boundary level without going into complete remission (HAM-A > 7 points).
Depression changes during the treatment
At a baseline mean HAM-D scores in F and JD patients were 20,9 ± 6,2 and 23,3 ± 7,4 respectively. At week 4 during the treatment more significant reduction of depressive symptoms was observed in patients with fibromyalgia, who received psychopharmacotherapy. In particular, mean HAM-D scores were estimated at 12,7 ± 4,1. In JD-Ph and F-Ps groups mean HAM-D scores were nearly identical and estimated at 15,4 ± 4,1 and 15,0 ± 4,4 points, respectively. At week 4 the highest depression level was noted in JD-Ps group (16,5 ± 4,3). In case of depression, statistically significant difference on this treatment stage was also demonstrated in favor of pharmacological treatment (p<0.05).
At the end of the treatment, the most significant reduction in depression symptoms was observed in all patients regardless of treatment type: mean HAM-D scores in F-Ph, F-Ps, JD-Ph and JD-Ps groups were estimated at 3.1 ± 2.4, 3,4 ± 2,6, 6.2 ± 3.2 and 7.1 ± 3.4 points, respectively. From these data, it can be seen that patients with fibromyalgia had more pronounced decrease in their depression symptoms.
Comparative effectiveness of psychopharmacotherapy versus psychotherapy in patients with chronic pain
While comparing psychopharmacotherapy effectiveness in patients with fibromyalgia and dorsalgia/joint pain, we have identified statistically significant differences in reduction of HAM-A scores between both in the short-term (MD 13.5 vs. 8.5; p = 0.008) and for the entire treatment period (MD 18.9 vs. 15.3; p = 0.033). Although, it wasn’t the case for treatment period between weeks 4-12, where the difference was not significant (p = 0.126).
As for psychotherapy, on the contrary, we hadn’t found any statistically meaningful difference in anxiety level improvement between patients with fibromyalgia and dorsalgia/joint pain during the initial treatment period (p = 0.478). But the difference became significant during the second treatment period (12.6 vs 8.3; p = 0.045) and entire treatment (20.4 vs 15.1; p = 0.036).
Comparative analysis of treatment effectiveness in patients with fibromyalgia has shown statistically significant difference in favor to pharmacotherapy compared to psychotherapy for 1st treatment period (MD 13.5 vs. 7.8; p = 0.026). But for the 2nd treatment period, from week 4 to 12, such difference, in contrast, was noted for psychotherapy, compared to pharmacotherapy (MD 12.6 vs. 5.4; p = 0.008). In the long-term, both treatments were equally effective (Table 1).
Analysis didn’t demonstrate any significant statistical differences in anxiety improvement between patients with joint pain/dorsalgia, who received pharmacotherapy or psychotherapy, nor between baseline and week 4 or from week 4 to week 12 (Table 1).
| Treatment period | Treatment type | Mean difference | 95% Confidence interval | P |
| Fibromyalgia | ||||
| Baseline — week 4 | Pharmacotherapy | 13.5 | 10.2-16.8 | 0.026* |
| Psychotherapy | 7,8 | 6.3-9.3 | ||
| Week 4 to 12 | Pharmacotherapy | 5.4 | 4.2-6.6 | 0.008* |
| Psychotherapy | 12.6 | 10.1-15.1 | ||
| Overall, baseline — week 12 | Pharmacotherapy | 18.9 | 16.1-21.4 | 0.363 |
| Psychotherapy | 20.4 | 17.3-23,5 | ||
| Joint pain and dorsalgia | ||||
| Baseline — week 4 | Pharmacotherapy | 8.5 | 5.3-11.7 | 0.328 |
| Psychotherapy | 6.8 | 5.2-8.4 | ||
| Week 4 to 12 | Pharmacotherapy | 6.8 | 4.7-8.9 | 0.262 |
| Psychotherapy | 8.3 | 5.7-10.9 | ||
| Overall, baseline — week 12 | Pharmacotherapy | 15.3 | 12.4-18.2 | 0.652 |
| Psychotherapy | 15.1 | 12.0-18.2 | ||
On the contrary to anxiety, depressive symptoms' improvement didn’t differ significantly between patients with fibromyalgia and those with chronic pain of other etiology. Thus, psychopharmacotherapy efficiency with respect to depressive symptoms, evaluated by HAM-D, had similar effectiveness for the first (p = 0.456), second (p = 0.621), and entire treatment period (p = 0.542).
The same picture was observed and for psychotherapy effectiveness between patients with fibromyalgia and joint pain/dorsalgia. Borderline statistically meaningful difference was noted only for 2nd treatment period (p=0.041) with more pronounced improvement in patients with fibromyalgia (11.6 vs. 9.4), but not for overall treatment course (p=0.442).
Comparative analysis between psychotherapy and psychopharmacotherapy for fibromyalgia has demonstrated statistically significant difference in improvement of depression symptoms in favor of latter treatment type for the first treatment period (5.9 vs. 8.2; p = 0.048), but in favor of psychotherapy for time period between week 4 and 12 (9.6 vs. 11.6; p = 0.016). Overall improvement was equal between these treatment types. As for comparative treatment effectiveness in patients with chronic pain/dorsalgia, there weren’t any difference noted in all treatment periods (Table 2).
| Treatment period | Treatment type | Mean difference | 95% Confidence interval | P |
| Fibromyalgia | ||||
| Baseline — week 4 | Pharmacotherapy | 8.2 | 7.1-9.3 | 0.048* |
| Psychotherapy | 5.9 | 4.8-7.0 | ||
| Week 4 to 12 | Pharmacotherapy | 9.6 | 8.1-11.1 | 0.016* |
| Psychotherapy | 11.6 | 10.2-13.0 | ||
| Overall, baseline — week 12 | Pharmacotherapy | 17.8 | 14.9-20.7 | 0.547 |
| Psychotherapy | 17.5 | 15.1-19.9 | ||
| Joint pain/dorsalgia | ||||
| Baseline — week 4 | Pharmacotherapy | 7.9 | 5.8-9.0 | 0.278 |
| Psychotherapy | 6.8 | 5.2-7.4 | ||
| Week 4 to 12 | Pharmacotherapy | 9.2 | 7.7-10.7 | 0.424 |
| Psychotherapy | 9.4 | 8.1-10.7 | ||
| Overall, baseline - week 12 | Pharmacotherapy | 17.1 | 14.2-20.0 | 0.348 |
| Psychotherapy | 16.2 | 13.4-19.0 | ||
Conclusion
As can be seen from the study results, effects from pharmacotherapy regarding anxiety and depression improvements was more significant in short-term after treatment start, compared to psychotherapy. But in the long term, at week 12, effectiveness of these treatment types was similar.
This pattern was seen mostly in patients with fibromyalgia, but not for those with joint pain and dorsalgia. In latter patients for the entire treatment course effectiveness of psychotherapy and pharmacotherapy was also nearly identical.
Overall, these data indicate similar effectiveness of pharmacotherapy and psychotherapy in treatment of anxiety and depression symptoms in patients with chronic pain.